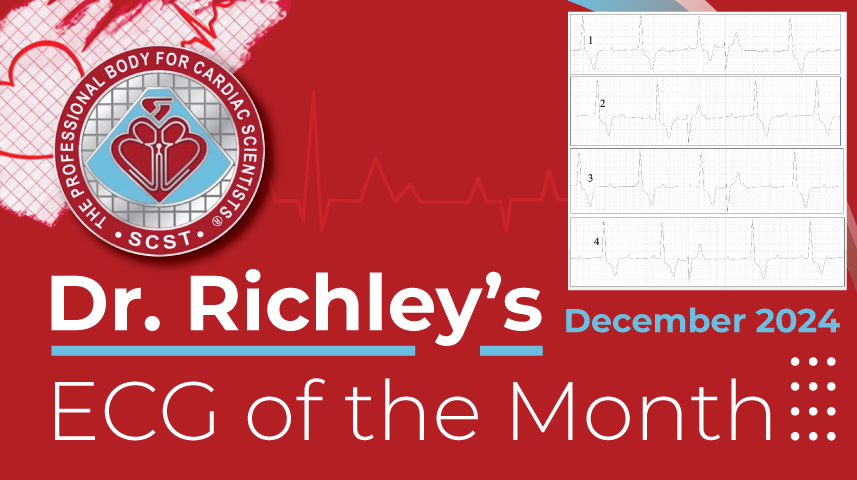
Arrhythmia time again. Below are four strips from a 24-hour ambulatory ECG recording. What exactly is going on here?
Dr Dave Richley

Answer Added 30.11.24
It seems from the responses received that the two most popular explanations for what we see are (1) complete heart block with a ventricular escape rhythm and ventricular premature beats (VPBs), and (2) high-grade AV block with a ventricular escape rhythm and occasional conducted beats.
There seems to be agreement that there is AV block that is at least high-grade and perhaps complete. The main question then is whether the relatively early beats are VPBs or conducted beats. I think they are conducted beats because they have in common that:
(1) they follow a P wave with PR intervals that are very similar, and
(2) the P waves preceding the early premature QRS complexes all occur in the same part of the cardiac cycle, very close to the end of the preceding T wave.
So, if the early QRS complexes do indeed represent conducted beats, why should these particular sinus impulses, which are early, manage to conduct when most others do not? Normally, in high-grade AV block, where the majority of sinus impulses fail to conduct, we expect conduction to take place only after a sufficiently long RP interval that the conduction system has had time to recover.
The answer to this apparent paradox is supernormal conduction. Supernormal conduction is not a recently discovered phenomenon. It has been known about for over a century and it refers not, as the name would suggest, to conduction that is better than normal, but to conduction that is transiently better than expected in someone who has impaired conduction. There is a very brief period in which supernormal conduction can occur and this is just before the end of repolarisation (phase 3 of the action potential), when the membrane potential is just above the threshold potential before it returns to its resting level. A stimulus at this point in the cardiac cycle can elicit a new action potential whereas a stimulus just before or just after this point will not. This brief period corresponds to a position near the end of the T wave on the ECG. So, a sinus impulse that arrives at the ventricles just before they have repolarised completely, may elicit a new depolarisation and therefore be conducted. It is of note that the property of supernormal conduction appears to be possessed only by the bundle branch system and not by the AV node or atrial or ventricular myocardium.
In this ECG all the conducted beats have the same broad QRS morphology, so I think they show a bundle branch block, although it is not possible from this single-channel recording to determine which bundle branch is blocked. However, what this means is that the other bundle branch shows supernormal conduction when the sinus impulse arrives at the right moment.
The Wedensky effect and Wedensky facilitation have also been credited with unexpected increased conduction and excitation but, while I am most definitely not an expert on the various Wedensky phenomena, I don’t think that they apply in this case. The Wedensky effect is seen when a large suprathreshold stimulus causes a following stimulus which would normally be sub-threshold to result in the initiation of an action potential. This effect has been demonstrated in human hearts in experimental conditions with electronic pacing stimuli: a pacing stimulus that is too small to be effective normally can be made to be effective and produce a QRS if it is preceded by a much greater stimulus that results in ventricular excitation. This phenomenon does not have the same relationship to the period of supernormal conductivity described above, tending to occur some time after the end of the T wave. Wedensky facilitation is the phenomenon whereby the arrival of an impulse proximal to an area of block can improve conduction beyond the block by lowering the excitability threshold of the post-block tissue through the process of electrotonic potentiation or modulation. Again, I don’t think this is the explanation for what we see in the ECG strips.
Anyone who wishes to further explore the topics of supernormal conduction and the Wedensky phenomena may find the papers detailed below useful.
I have now exhausted my supply of appropriately challenging ECGs, so no more ‘ECG of the Month’ features are planned. I wish to thank everyone who has been kind enough to contribute ECGs as well as those who have participated in the discussions. I hope the series has been of some interest and educational benefit.
Recommended reading:
Castellanos A, Emberg L, Johnson D, Berkovits BV. The Wedensky Effect in the Human Heart. Heart 1966;28:276-283. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC459069/pdf/brheartj00331-0134.pdf
Elizari MV, Schmidberg J, Atienza A, Paredes DV, Chiale PA. Clinical and experimental evidence of supernormal excitability and conduction. Curr Cardiol Rev. 2014 Aug;10(3):202-21. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4040872/
Hnatkova, K., Malik, M. Noninvasive Wedensky Modulation. Card Electrophysiol Rev 1999;3: 269–273.
sinus bradycardia, QRS – LBBB morphology , AV 3rd degree (complete heart block), VE’s
Thanks Paulina. I think what you say is plausible but when I study the precise timing of the events I wonder if there might be an alternative explanation. Let’s see what others think.
I think it may be 3rd degree with two competing ventricular escape rhythms but I also feel I’ve missed something obvious and second guessing myself!
Thanks Merry. Well, there certainly seems to be one ventricular escape rhythm but of the two QRS morphologies one appears early so probably shouldn’t be considered an escape beat.
Ah then one escape rhythm with a VEs coming from a second focus within the ventricles, perhaps
Well, they all seem to follow a VE (ventricular extrasystole) that has a coincidental, but not conducted, PR sequence. My guess would be those ventricular complexes don’t retrograde conduct quite as far back up, the AV being it’s still partially refractory from incomplete anterograde conduction of the prior P wave, so when the next P wave arrives both the upper and lower AV have had a relatively longer recovery time. Or something like that.
That’s not something I’d thought of so I’ll have another look.
Possible, but I think there’s another, possibly more plausible, explanation.
Sinus bradycardia with a third degree AV block in the presence of a ventricular escape rhythm, and premature ventricular ectopics. Or this could be some type of higher grade AV block, some p-p intervals look regular and some irregular and some beats have possible 1:1 conduction with variable PR intervals but this may be pure coincidence. The R-R interval also measures regular in some intervals but is but is irregular due to some VEs. There may also be an element of iso-rhythmic AV dissociation in some beats also due to very similar A and V rates but overall hard to determine.
Sorry Joe – I missed this when you posted it. You’ve summarised some of the observations and possibilities but I don’t think there’s any isorhythmic AV dissociation because the atrial and ventricular rates seem very different to me.
CHB, occasional AVC
Thanks, Scott. What is an AVC?
Atrio-Ventricular Conduction.
Ah, right. So why might those particular impulses be conducted when others aren’t?
I am sure there is an AV dissociation and PVCs
Thanks, Osama. You could be right, but are the early beats definitely PVCs?
Sinus rhythm with rate of 85-ish bpm.
Complete heart block with slow ventricular escape rhythm, resulting in marked bradycardia with rate of 35-ish bpm.
Premature ventricular complexes also noted.
Thanks, Adriano. I’m wondering if the premature impulses are definitely of ventricular origin. I suspect they are not!
Wedensky facilitation
Thanks, wangchangkun. Would you care to provide a bit of explanatory detail for the benefit of readers?
Feels simple enough but knowing you, I’m probably missing something.
As all four strips appear to show the same pathology, I’ll just focus on strip #1:
1. There is a regular interrupted sinoatrial rhythm ≈ 83/min.
2. What initially seems like CHB with a ventricular escape rhythm is interrupted by a different-looking beat (R4) which arrives earlier than expected, suggesting it is conducted. The PRI appears to be stable for similar beats in the other strips (R3 in strips 2 and 4; R4 in strip 3).
3. As there is occasional AV conduction, we can call high-grade AV block.
In strip #1, I can’t help but notice how different R3 looks from the other ventricular escape beats — not completely accounted for by the brief period of baseline wander. I do not think it is truly (functionally) different from the rest.
Thanks, Onyinye. I think the question is: if the premature beats are conducted, why are they conducted when other impulses are not?
Best explanation would be the Wedensky effect, methinks.
Most recent example I’ve seen is this:
https://x.com/syamkumarmd/status/1842350133729460630?t=PY2ArxoAuhUKOe2vvUWY0A&s=19
I think we’re thinking along similar lines.
Could someone please summarise Wedensky Effect vs Facilitation vs Inhibition or direct us to a review on this topic?
Good request, Jeff. I’ll see what I can find and maybe there are others who can help out.
CHB with aberrantly conducted SVEs?
No SVE, I mean VEs.